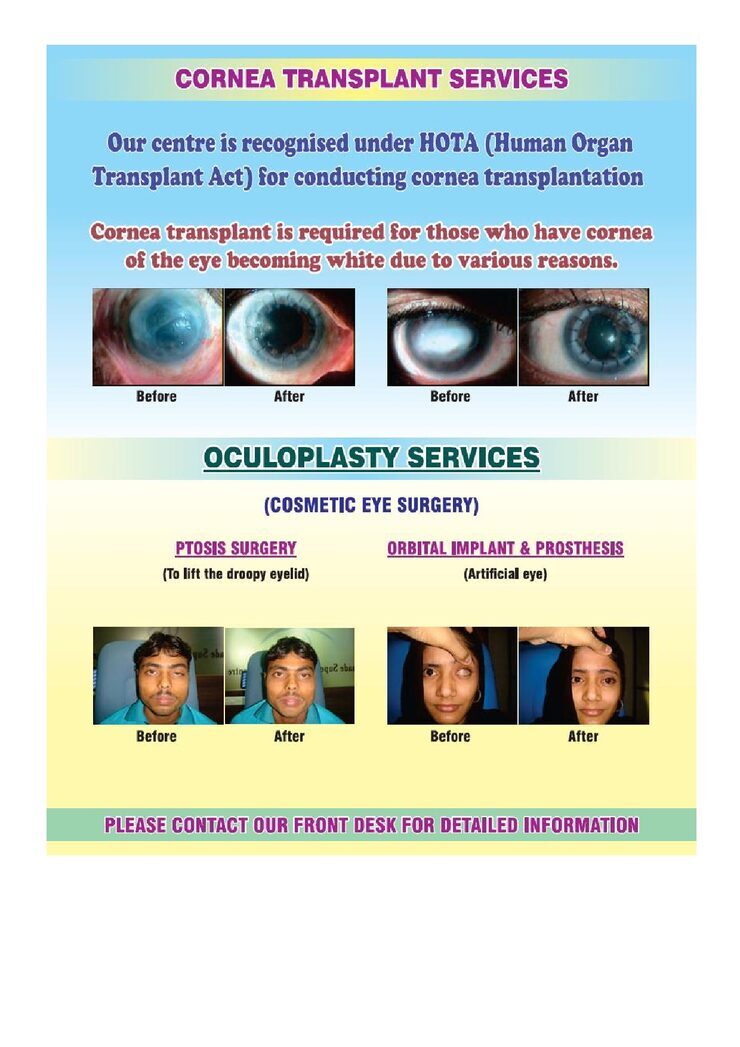
CORNEA TRANSPLANT SURGERY
The hospital has advanced facilities to conduct the most difficult of the Cornea Transplant surgeries with immense ease.
The Hospital also has to its credit the Youngest ever successful Cornea Transplant done in India- for a child of 4 months old.






CONGENITAL PTOSIS ( DROOPY EYE-LIDS)
What is Eyelid Ptosis ?
A drooping eyelid is called ptosis or blepharoptosis. In ptosis, the upper eyelid falls to a position that is lower than normal. In severe cases of ptosis, the drooping eyelid can cover part or all of the pupil and interfere with vision, resulting in amblyopia.
All pediatric patients presenting with either unilateral droopy eyelid or bilateral droopy eyelids need a thorough examination that includes a medical history, a family history, a history of drug or allergic reactions, and a review of systems.Family photographs can help determine onset or variability of the ptosis.
TREATMENT Options-
- Observation is only required in mild cases of congenital ptosis if no signs of amblyopia, strabismus, and abnormal head posture are present.
- Depending on the severity of the congenital ptosis, patients should be monitored every 3-12 months for signs of amblyopia due to congenital ptosis. External photographs can be helpful in monitoring patients.
- Head posture should be carefully examined. If the patient acquires a chin-up posture due to the worsening of ptosis, surgery may be indicated.
- The patient should be checked for astigmatism due to the compression of the droopy eyelid.
Congenital ptosis has physical, functional, and psychological consequences. The method of repair depends on treatment goals, the underlying diagnosis, and the degree of levator function. Although the primary reason for the repair is functional, the surgeon has an opportunity through this procedure to produce symmetry in lid height, contour, and eyelid crease for better cosmesis.
- Surgical correction of congenital ptosis can be undertaken at any age depending on the severity of the disease.
- Earlier intervention may be required if significant amblyopia or ocular torticollis is present.
- Severe cases of ocular torticollis may delay mobility in infants and toddlers because of the balance problems from extreme chin-up head posture.
- If intervention is not urgent, surgery is often delayed until age 3-4 years. Waiting until this age allows for more accurate measurements pre-operatively.
Surgery for ptosis in patients with a history of dry eyes, seventh cranial nerve palsy, or significant extraocular muscle abnormalities, such as severe Graves ophthalmopathy, double elevator palsy, or progressive external ophthalmoplegia, should be approached with great caution to avoid exposure keratopathy following the surgery.
Levator muscle resection
This procedure is the shortening of the levator-aponeurosis complex through a lid-crease incision. The skin incision is hidden either in the existing lid fold or in a new lid fold created to match that of the contralateral eyelid.
Moderate levator function must be present to offer a chance for correction with a levator resection. If the levator function is greater than 4 mm but less than 6 mm, a levator resection of greater than or equal to 22 mm is recommended. If the levator function is 6-8 mm, a levator resection of 16-18 mm is indicated. If the levator function is greater than 8 mm, a levator resection of 10-13 mm is indicated.
Contraindications: An external levator resection is not indicated when the levator function is less than 4 mm. In such cases, a long-term surgical outcome may result in undercorrection. Poor Bell phenomenon (limited elevation of the eye), reduced corneal sensitivity, or poor tear production can produce exposure keratopathy.
Frontalis suspension procedure
This procedure is designed to augment the patient's lid elevation through brow elevation. Frontalis suspension procedures produce lagophthalmos in most cases. Some surgeons prefer to perform a bilateral suspension procedure for severe unilateral congenital ptosis to obtain symmetry.
The procedure is indicated when the levator function is less than 4 mm.
Relative contraindications are poor Bell phenomenon (limited elevation of the eye), reduced corneal sensitivity, or poor tear production, which can produce exposure keratopathy. If surgery is still indicated, these patients need close postoperative follow-up care to avoid corneal exposure, infection, corneal ulcer and amblyopia.
Several materials are available to secure the lids to the frontalis muscles.[10, 11, 12, 13] These materials include the following:
-
Autogenous fascia lata: Autogenous fascia lata can be obtained from the leg of patients older than 3 years.
-
Preserved (tissue bank) fascia lata
-
Nonabsorbable suture material (eg, 2-0 Prolene, Nylon (Supramid) or Mersilene)
-
Silicone bands, silicone rods
-
ePTFE (expanded Poly Tetra Fluoro Ethylene), Gore-Tex
-
Autogenous materials used less frequently include palmaris longus tendon and temporalis fascia.
Patients may not be able to close their eyelids during sleep from a few weeks to several months following surgery. Families must be warned of this outcome before the operation. The problem of open lids during sleep improves with time; however, aggressive lubrication is needed to avoid exposure keratopathy.
Fasanella-Servat procedure
The upper lid is elevated by removing a block of tissue from the underside of the lid. This tissue includes the tarsus, conjunctiva, and Müller muscle. This procedure is not commonly performed for cases of congenital ptosis.
Mueller muscle–conjunctival resection
This surgery is chosen if the eyelid has had a good response to phenylephrine. The conjunctiva and the Müller muscle are marked off, clamped, and sutured. The tissues are resected. Then, the conjunctival layer is closed. This procedure is not commonly performed for cases of congenital ptosis.
Visits
363937
269384

WORLD CLASS TECHNOLOGY
FOR ADVANCED RETINA & GLAUCOMA
DIAGNOSTICS
(TOPCON- JAPAN)

9321442297
9136028098
9136028035
022-25425411
022-25425422
022-25425433
